Cancer Education and Research Institute® (CERI)'s Cancer Education Programs
Our Team of cancer experts at Cancer Education and Research Institute® (CERI)'s, formerly Cancer Research Simplified, provides you with the most reliable, most up-to-date, and simplified cancer information available. Our educational programs quickly became trusted and highly sought after worldwide.
CERI strongly stands behind the importance of cancer patient empowerment and is a worldwide leading source for simplified, multi-language cancer education. Knowledge is power and empowerment is the key for greater treatment success, early diagnosis, as well as cancer prevention.
For any questions or requests, please submit your inquiry at our CERI Personalized Patient Program™ page.
CERI strongly stands behind the importance of cancer patient empowerment and is a worldwide leading source for simplified, multi-language cancer education. Knowledge is power and empowerment is the key for greater treatment success, early diagnosis, as well as cancer prevention.
For any questions or requests, please submit your inquiry at our CERI Personalized Patient Program™ page.
Glioblastoma Treatment
Aygün Sahin, MSc, PhD | CEO, President, and Cancer Lead, Cancer Education and Research Institute (CERI)
What is Glioblastoma?
Malignant gliomas are the most common malignancy in primary brain tumors (brain cancers that first occur in the brain. Brain cancers that occur due to metastasis of other cancer types in the body are called secondary brain tumors.).
Gliomas are are characterized by rapid growth with invasion into the surrounding brain parenchyma (supportive tissue).
Although malignant gliomas rarely metastasize to a distant location of the body, the invasive nature makes it very difficult to fully remove the tumor to cure the disease.
The tumor often recurs after surgery.
The most aggressive and deadly type of malignant gliomas is called glioblastoma multiforme (GBM). The median survival of the patients with GBM remains poor (~15 months) even after two decades of remarkable progress in surgery, chemotherapy, and readiotherapy.
Multimodality treatment involving surgery, radiation therapy, and chemotherapy is an accepted therapeutic strategy for GBM.
Gliomas are are characterized by rapid growth with invasion into the surrounding brain parenchyma (supportive tissue).
Although malignant gliomas rarely metastasize to a distant location of the body, the invasive nature makes it very difficult to fully remove the tumor to cure the disease.
The tumor often recurs after surgery.
The most aggressive and deadly type of malignant gliomas is called glioblastoma multiforme (GBM). The median survival of the patients with GBM remains poor (~15 months) even after two decades of remarkable progress in surgery, chemotherapy, and readiotherapy.
Multimodality treatment involving surgery, radiation therapy, and chemotherapy is an accepted therapeutic strategy for GBM.
Time Points for Chemotherapy in Glioblastoma Patients
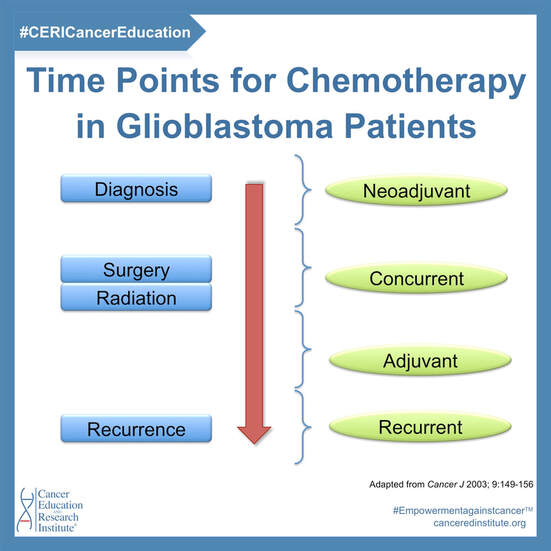
- Neoadjuvant therapy: Chemotherapy for GBM patients may be given before surgery and/or radiation therapy
- Concurrent therapy: Chemotherapy may be given at the time of surgery and/or radiation
- Adjuvant therapy: Chemotherapy may be given after surgery and/or radiation
- Recurrent therapy: Chemotherapy may be given at recurrence.
Chemotherapy Mechanisms in Glioblastoma
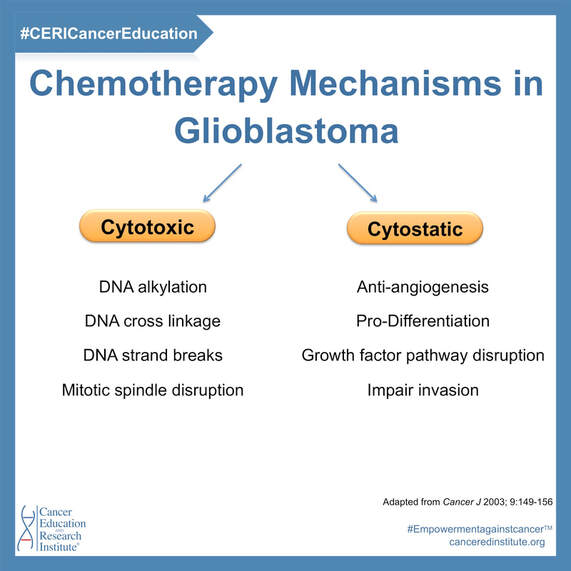
Glioblastoma multiforme (GBM) chemotherapies can be largely classified as cytotoxic or cytostatic.
In general, this is how the mechanism of action work with these therapeutic agents:
Increasingly, cytotoxic agents are being combined with cytostatic agents.
First-line systemic Cytotoxic agents:
Second-line systemic Cytotoxic agents:
Cytotatic agents:
In general, this is how the mechanism of action work with these therapeutic agents:
- Cytotoxic agents impair cell division by disrupting DNA synthesis and/or mitotic mechanisms.
- Cytostatic agents alter aspects of tumor biology to make the tumor behave less aggressively but do not necessarily kill tumor cells.
Increasingly, cytotoxic agents are being combined with cytostatic agents.
First-line systemic Cytotoxic agents:
- Temozolomide
- BCNU
- PCV (Procarbazine, CCNU, and Vincristine)
Second-line systemic Cytotoxic agents:
- Carboplatin
- VP-16 (Etoposide)
- CPT-11 (Irinotecan)
Cytotatic agents:
- cis-Retinoic Acid
- Thalidomide
- Tamoxifen
- Celecoxib
References:
- Parney, IF and Chang, SM. Current Chemotherapy for Glioblastoma. Cancer J 2003; 9:149-156
- Kondo, Y et al. Molecular targeting for malignant gliomas. Intl J Onc 2004; 24:1101-1109.
- Dunn IF and Black PM. The neurosurgeon as local oncologist: cellular and molecular neurosurgery in malignant glioma therapy. Neurosurgery 2003; 52: 1411-1422.
Do you need help with cancer diagnosis?
Please fill the application form on our CERI Personalized Patient Program page - we CAN help you!
#Empowermentagainstcancer™ #CERICancerEducation #CERICares #CancerSimplified
#cancer #glioblastoma #gbm #glioblastomatherapy #GBMtherapy #glioblastomatreatment #GBMtreatment #cancereducation #cancerresearch #cancertreatment #canceredinstitute
GET YOUR FREE ARTICLE: Make sure to get your free article as our gift to you! Go to: canceredinstitute.org/ceri-simplified-cancer-research-articles
CORONAVIRUS PAGE: For our educational and up-to-date informational page on Coronavirus, go to: canceredinstitute.org/coronavirus
FOLLOW US for DAILY information and updates:
CORONAVIRUS PAGE: For our educational and up-to-date informational page on Coronavirus, go to: canceredinstitute.org/coronavirus
FOLLOW US for DAILY information and updates:
- INSTAGRAM: instagram.com/canceredinstitute
- FACEBOOK: facebook.com/canceredinstitute
- Twitter: twitter.com/canceredinst
- LinkedIn: linkedin.com/company/canceredinstitute
You might also like:
|
|
|
Disclaimer: We can not assume responsibility of misinterpretation of content.
Please donate to support our program - help us save MORE lives!



